Patient Driven Payment Model (PDPM) Overview
- Overview also available in Portable Document Format (PDF)
ACRONYMS USED IN THIS PRESENTATION
- CMI
Case-Mix Index; a weight assigned to a specific Resource Utilization Group or an average for a given population - MDS
Minimum Data Set; a core set of screening, clinical and functional elements, specific instructions and schedule of assessments - PDPM
Patient Driven Payment Model; for Medicare Part A SNF resident stays only; replaced RUG-IV 10/1/2019 - ICD-10-CM
International Classification of Diseases, Tenth Revision, Clinical Modification - PPS
Prospective Payment System; a case-mix methodologyused to classify SNF residents in a Medicare-coveredPart A stay for payment purposes - RUG-III, RUG-IV
Resource Utilization Group, Versions III and IV, a nursing facility resident classification system used in case-mix reimbursement methodology - ADL
Activities of Daily Living; a component of the RUG calculation indicating the level or functional assistance of support required by the resident (replaced with functional score in PDPM) - UPL
Annual Medicaid demonstration required to ensure payments do not exceed the Medicare Upper Payment Limit
What is PDPM?
FY 2019 SNF PPS Final Rule (CMS-1696-F)
Effective 10/1/19
On July 31, 2018, the Centers for Medicare and Medicaid Services (CMS) published the FY 2019 SNF PPS Final Rule (CMS-1696-F), which included three major provisions:
- Changed the SNF Value-Based Purchasing Program;
- Changed the SNF Quality Reporting Program (QRP); and
- Changed the case mix classification system used under the SNF Prospective Payment System (PPS), which included implementation of a new case mix model, the Patient-Driven Payment Model (PDPM).
State Medicaid Director’s Letter (SMD# 22-005)
Released 9/21/2022
This letter, coupled with the release of draft minimum data set (MDS) changes on September 1 had several implications for state Medicaid programs and their nursing facility (NF) reimbursement systems.
- Beginning October 1, 2023, MDS items necessary for resident classification under a resource utilization group (RUG) based acuity system (RUG-III and RUG-IV) are no longer available on the standard MDS item sets.
- Allowed for the use of an optional state assessment (OSA) through September 30, 2025.
- CMS provided guidance related to the use of a patient-driven payment model (PDPM) approach for required annual upper payment limit (UPL) demonstrations. Guidance requires use of only PDPM components that align with services included in the Medicaid NF per diem rate.
What is PDPM?
Patient Driven Payment Model
- New case mix classification methodology that reimburses for a Medicare stay in a nursing facility based on the resident’s condition and resulting care needs, instead of based merely on volume of services.
- Incorporates 5 individual case mix adjusted rate components and 1 non-case mix adjusted component.
- Focuses on clinically relevant factors by using ICD-10 diagnosis codes and other resident characteristics as a basis for classification.
*Source: Acumen Skilled Nursing Facility Patient-Driven Payment Model Technical Report (April 2018)
Why PDPM?
Patient Driven Payment Model
- Adjusts Medicare payments based on each aspect of a residents care in order to more accurately address costs associated with medically complex residents.
- Focuses resident classifications on the expected needs of the residents rather than the volume of therapeutic services provided.
- Enhances payment accuracy for all SNF services. SNF residents who may have significant differences in terms of nursing needs and costs may receive the same payment for nursing services under a RUG methodology.
- Reduces PPS assessment administrative burden
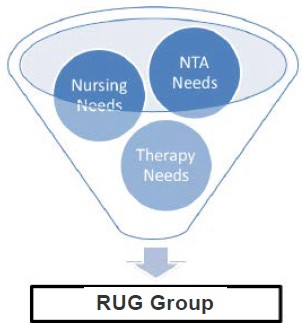
RUG Reimbursement Model
Volume Based Reimbursement
- Rate built upon the volume of potential therapy services provided to the resident.
- Consistent rate for the resident's Part A stay, unless assigned to another RUG score.
- Rate calculation includes:
- Two case mix adjusted components: Therapy and Nursing
- One Non-Case-Mixed Base Rate Component
- Nursing CMI Includes cost of: Nursing, Social Services, and NTA
- Therapy CMI includes cost of: PT, OT, SLP
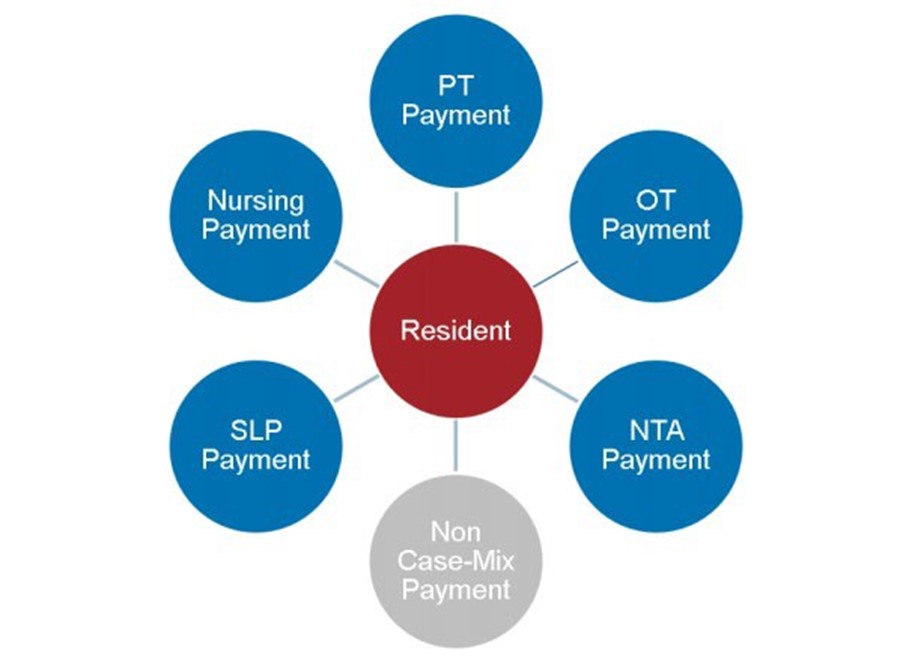
PDPM Reimbursement Model
Resident Characteristic Driven Model
- Rate built upon resident characteristics, not volume of services, and designed to better meet individual care needs.
- Certain rate components include a variable per diem adjustment.
- Rate calculation includes:
- Five Case-Mix Adjusted Components: PT, OT, SLP, Non-Therapy Ancillary, & Nursing
- One Non-Case Mixed Base Rate Component

- Five Case-Mix Adjusted Components: PT, OT, SLP, Non-Therapy Ancillary, & Nursing
- One Non-Case Mixed Base Rate Component
Source: CMS Presentation, "Patient Driven Payment Model: Background & Finalized Changes to the Skilled Nursing Facility (SNF) Prospective Payment System (PPS)"
Rationale for Additional Payment Groups
Patient Driven Payment Model
- PT and OT resident needs were found to be closely correlated to each other, however SLP resident needs were not.
- Predicted resident PT and OT costs were shown to gradually reduce over time as the resident regains functioning. Predicted resident SLP costs did not.
- The stand alone nursing component allows for reimbursement to align solely with nursing resource use and will no longer be distorted by the number of therapy minutes provided.
- Non-Therapy Ancillary (NTA) resident needs vary greatly by resident and case mix group, and a separate component allows for reimbursement to better align with need. Predicted resident NTA cost were not strongly correlated with previous Nursing/Therapy RUG weights.
- Predicted NTA costs were found to be front-loaded in a residents stay.
PDPM Resident Classification
Basis for Resident Classification:
- Physical Therapy (PT)
Clinical Category, Functional Score
Under PDPM, resident characteristics will be used to predict the therapy costs associated with a given resident, rather than rely on service use - Occupational Therapy (OT)
Clinical Category, Functional Score
Under PDPM, resident characteristics will be used to predict the therapy costs associated with a given resident, rather than rely on service use - Speech Language Pathology (SLP) Presence of Acute Neurologic Condition, SLP-related Comorbidity or Cognitive Impairment, Mechanically-altered Diet, Swallowing Disorder used to predict costs
- Non-Therapy Ancillary (NTA)
NTA Comorbidity Score- Comorbidities associated with high increases in NTA costs grouped into various point tiers
- Points assigned for each additional comorbidity present, with more points awarded for higher-cost tiers
- Nursing
Same characteristics as under RUG-IV, with certain modifications.- Function score based on Section GG of the MDS 3.0
- Collapsed functional groups, reducing the number of nursing groups from 43 to 25.
- Variable Per Diem Adjustment
For the PT, OT, and NTA components, the case-mix adjusted per diem rate is multiplied against the variable per diem adjustment factor, following a schedule of adjustments for each day of the resident's stay
Nursing Component
- The nursing component continues to serve as the payment mechanism for nursing and social services. Under PDPM, the NTA services have been segregated from the nursing component.
- The basis for the nursing component case mix weights continues to be the 2006/2007 STRIVE time studies.
- PDPM case mix groups were generated by collapsing the RUG-IV 66 grouper methodology.
- The rehabilitation groupings were removed (covered by new PT/OT/SLP components). The remaining 43 groups were further modified by eliminating certain ADL functional score groupings.
- ADL functional score basis are transitioned from MDS section G to MDS section GG. Due to this transition, there is no direct crosswalk of groupings.
What's Included?
Nursing Component
2006-2007 Strive Study
- RN/LPN/CNA*
- Respiratory Therapist
- Certified Medication Aide
- Restorative Aide
- Bath Aide
- Psych Aide
- Non-Certified Tech
- Clinical Associate
- Transportation
- RT Assistant
*Encompasses the majority of time measured
NTA and Non-Case Mix
Non-Therapy Ancillary (NTA) Non-Case Mix
- Drugs and Medications*
- Respiratory and Therapy Services
- Inhalation Services
- Other Respiratory
- IV Therapy
- IV solutions
- Laboratory
- Radiology
- Medical Supplies
- Surgical Supplies
*Drugs make up majority of NTA cost considerations
Non-Case Mix
- Room and Board*
- Administrative*
- Capital
*Makes assumption that Food, Dietary, Maintenance, Housekeeping, Laundry, Activities, and Medical Records fall under non-case mix component as either Room and Board or Administrative
IMPACT OF MEDICAID POPULATION ON PDPM DECISIONS
CURRENT COMPONENTS OF DIRECT COMPONENT
Overview
- Direct component of the rate includes:
- Nursing Administration
- Activities
- Social Service
- Transportation
- Physical Therapy
- Occupational Therapy
- Speech and Hearing Therapy
- Pharmacy
- Central Service and Supply
- Residential Health Care Facility
MEDICAID DUAL ELIGIBLE IMPACT
Overview
- Dual eligible (Medicare/Medicaid) recipients encompass a significant portion of the Medicaid nursing home population.
- Payment responsibilities for Duals differ significantly from those for non-dual eligible recipients for items such as therapies and drugs.
- These payment responsibilities differences may impact the choice of PDPM components for a Medicaid payment system.
MEDICAID DUAL ELIGIBLE IMPACT
Primary Payer Summary
Medicare Part B
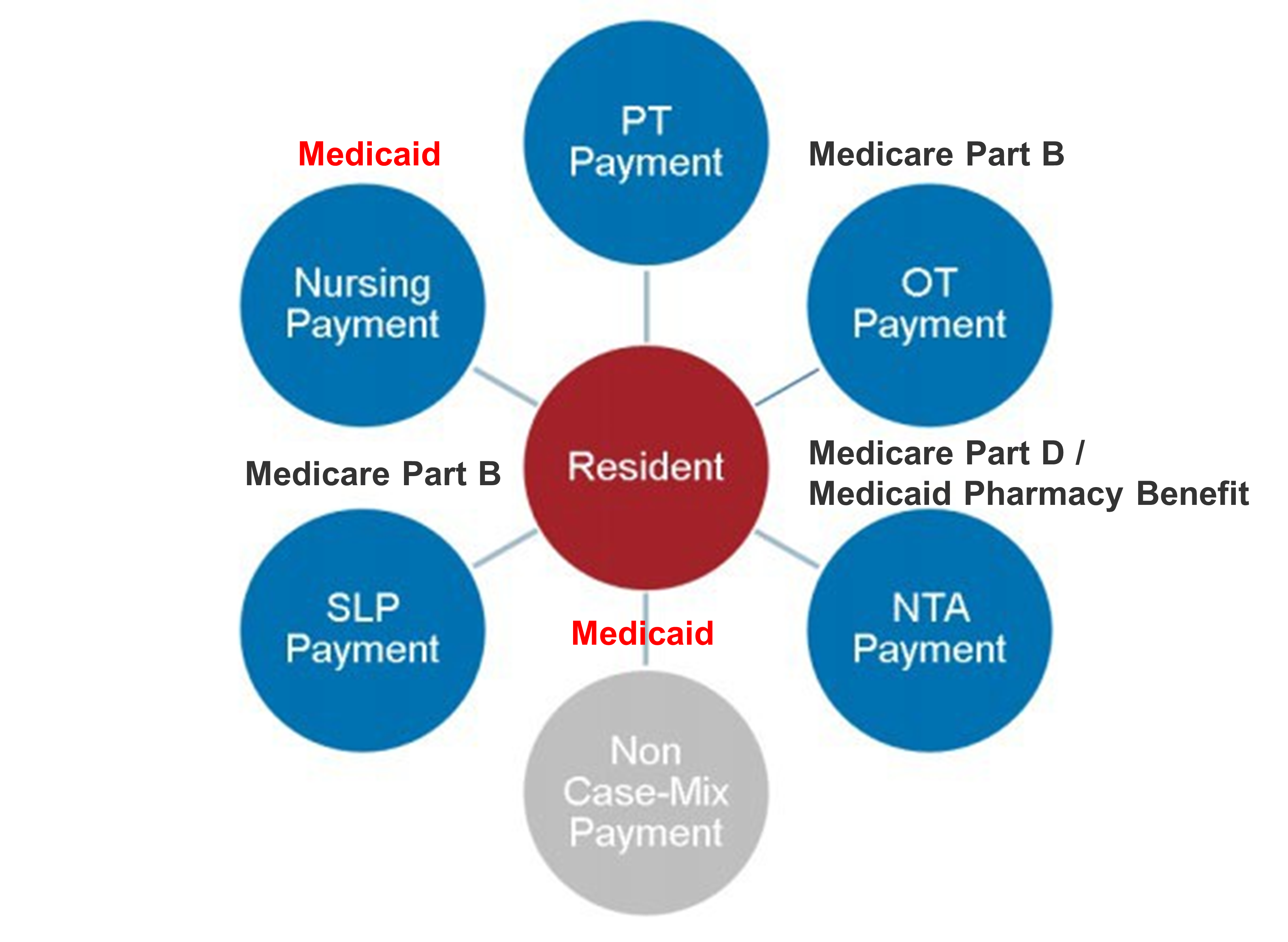
*Source (labels added by M&S): Acumen Skilled Nursing Facility Patient-Driven Payment Model Technical Report (April 2018)
Payment for Therapy Services
- Medicare Part B covers professional and non-inpatient services for beneficiaries. This benefit program provides payment for outpatient therapy services, and for recipients in NFs not on a Medicare Part A stay
- Medicare Part B pays for PT, OT, and SLP services for Medicaid dual eligible recipients after the conclusion of their Medicare part A stay.
- Medicare Part B therapy service caps were repealed through the Bipartisan Budget Act of 2018. The former therapy caps are now utilized as a threshold for when facilities must indicate in the medical record the medical necessity for additional therapy.
Payment for Prescription Drugs
- Medicare Part D is the Medicare prescription drug benefit program. Medicaid programs enroll dual eligible residents in this program.
- Medicare Part D pays for the majority of covered prescription drug costs for Medicaid dual eligible recipients in nursing facilities after the conclusion of their Medicare part A stay.
- Any prescription drugs not covered by Medicare part D are generally covered through the Medicaid pharmacy benefit, and not included within the Medicaid per diem.
CURRENT WORK
COMPLETED WORK SO FAR
Summary of Project Status
- Myers and Stauffer in process of obtaining rate setting and supporting cost information from the State
- CMS approval of required MDS Data Use Agreement (DUA) between the State and Myers and Stauffer still in process
- Signed DUA is necessary prior to Myers and Stauffer obtaining and utilizing MDS information for modeling, and as such Facility-wide and Medicaid PDPM CMI information is not yet available
MAJOR DECISIONS
Summary of Major Undecided Decision Points
- PDPM component usage for Medicaid CMI
- Nursing
- NTA: Non-Therapy Ancillary
- SLP: Speech Language Pathology
- OT: Occupational Therapy
- PT: Physical Therapy
- PDPM weight set to utilize
- Data to allow for state specific adjustments is not published
- Phase-in considerations
- Method to ensure facilities have appropriate time to adjust a new CMI
- Method and timing of phase-in
- Anticipated timeline for Implementation
- Initial targeted completion date is fall of 2025
- Stakeholder Workgroups and Meeting Schedules
CONTACT US
- Contact E-mail Address
NYNF@mslc.com
DEDICATED TO GOVERNMENT HEALTH PROGRAMS
