2022 Value Based Payment Reporting Requirements
Technical Specifications Manual
- 2022 Tech Spec Manual is also available in Portable Document Format (PDF)
____________________________________________________________
New York State Department of Health Email Address: OQPSVBP@health.ny.gov
HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).
____________________________________________________________
Last revised May 23, 2022
Table of Contents
- INTRODUCTION
- VBP ARRANGEMENTS AND ASSOCIATED QUALITY MEASURES
- CATEGORIZATION OF QUALITY MEASURES
- CLASSIFICATION OF QUALITY MEASURES
- ORGANIZATIONS REQUIRED TO REPORT
- MAINSTREAM & SUBPOPULATION VBP ARRANGEMENTS [OTHER THAN MLTC]
- MEASURE CHANGES
- WHERE TO SUBMIT VBP REPORTING DATA
- TABLE 1: 2022 VBP LIST OF REQUIRED MEASURES
- PATIENT ATTRIBUTION FILE
- MEASURE CHANGES
- TABLE 2: 2022 MLTC VBP LIST OF REQUIRED MEASURES
- MLTC ATTRIBUTION FILE
- ATTRIBUTION METHODOLOGY
- FILE FORMAT
- FIELD DEFINITIONS
- FILE SUBMISSION
- TABLE 3: 2022 VBP LIST OF CATEGORY 2 MEASURES
- TABLE 4: 2022 VBP MLTC CATEGORY 2 MEASURES
- TABLE 5: NYS FIPS CODES BY COUNTY
- TABLE 6: SUBMISSION EXAMPLES
- TABLE 7: MCO ATTRIBUTION FILE - DATA QUALITY CHECKLIST
- TABLE 8: MLTC ATTRIBUTION FILE - DATA QUALITY CHECKLIST
| Important Dates & Contact Information | ||||
|---|---|---|---|---|
| Mainstream VBP | MLTC VBP | |||
| Contact | OQPSVBP@health.ny.gov | Contact | MLTCVBP@health.ny.gov | |
| Submission Date | All files must be received electronically by 11:59 p.m. ET Friday, July 29, 2022. | Submission Dates | Plan/Provider-VBP Contractor performance to the State by July 22, 2022 | |
| MLTC VBP data files: All files must be received electronically by 11:59 p.m. ET Friday, July 29, 2022. | ||||
| Health Commerce System (HCS) | https://commerce.health.state.ny.us | Health Commerce System (HCS) | https://commerce.health.state.ny.us | |
| To: OQPS VBP Evaluation | To: MLTC VBP Evaluation | |||
I. Submission Requirements
INTRODUCTION
The purpose of this document is to make stakeholders aware of the quality measure reporting requirements for Medicaid Managed Care Organizations (MCOs) participating in the New York State Medicaid (NYS) VBP program. The 2022 Value Based Payment Reporting Requirements refer to 2021 Measurement Year (MY) data, except for Managed Long-Term Care plans, for which the reporting requirements refer to 2022 MY data.
Sections II, III, and IV of this document include guidance for the organizations responsible for reporting, the subset of measures for which reporting will be required by Mainstream VBP Arrangements and the changes to the reportable set of MY2021 Quality Measure Sets (see TABLE 1: 2022 VBP LIST OF REQUIRED MEASURES). Sections V and VI provide guidance for MLTC VBP Arrangements.
The New York State Department of Health (NYS DOH) has reached the completion of the first phase of a health transformation effort, known as the State Innovation Model (SIM) award, which focused on the transformation of primary care delivery and payment models statewide. The New York State Patient Centered Medical Home (NYS PCMH) model was created as part of the SIM initiative. With NYS PCMH, a Primary Care Core measure set was developed, and multi-payer data is used to calculate results for practices for the measure. To reduce the burden on MCOs participating in both the NYS PC measure set model and Medicaid VBP, we are aligning the reporting for both programs and utilizing the NYS Primary Care Core Set Scorecard data request to fulfill reporting requirements for both programs, where possible.
VBP ARRANGEMENTS AND ASSOCIATED QUALITY MEASURES
The VBP Roadmap outlines six types of VBP arrangements to be included for MY2021:
- Total Care for the General Population (TCGP) Arrangement: Includes all costs and outcomes for care, excluding certain subpopulations (specified below).
- Total Care for Special Needs Subpopulation Arrangements: Includes costs and outcomes of total care for all members within a subpopulation exclusive of TCGP.
- Children's Subpopulation: to address the unique needs of children at different developmental stages
- Behavioral Health/Health and Recovery Plans (HARP): for those with Serious Mental Illness or Substance Use Disorders
- People Living with HIV/AIDS
- Managed Long Term Care (MLTC)
- Episodic Care Arrangements:
- Maternity Care: Includes episodes associated with a pregnancy, including prenatal care, delivery and postpartum care through 60 days post-discharge for the mother, and care provided to the newborn from birth through the first 30 days post-discharge.
- IPC arrangements
CATEGORIZATION OF QUALITY MEASURES
Through a multi-group stakeholder engagement process, a set of quality measures was defined for each arrangement. Based on an analysis of clinical relevance, reliability, validity, and feasibility, each measure was placed into one of three categories:
- Category 1: Selected as clinically relevant, reliable, valid, and feasible. These measures are outlined in Table 1.
- REQUIREMENT: Only the Category 1 measures that are indicated in this document as "Required to Report" (✓) are to be reported by the MCO to the State.
- Category 2: Seen as clinically relevant, valid, and reliable, but where the feasibility could be problematic.
Category 2 measures are listed in the appendix (Table 3) of this guide. - Category 3: Rejected based on a lack of relevance, reliability, validity, and/or feasibility. These measures are not included in this manual.
CLASSIFICATION OF QUALITY MEASURES
Each Category 1 measure is classified as either Pay-for-Performance (P4P) or Pay-for-Reporting (P4R). Pay-for-Performance measures are intended to be used in the determination of shared savings amounts for which VBP Contractors are eligible. P4R measures are intended to be used by the MCOs to incentivize the VBP Contractors for reporting data to monitor the quality of care delivered to members in a VBP contract.
|table of contents|ORGANIZATIONS REQUIRED TO REPORT
Medicaid Managed Care Organizations with Level 1 or higher value-based contracting arrangements are required to report. All submissions must be received electronically by 11:59 p.m. ET on Friday, July 29, 2022.
|table of contents|REPORTING GUIDELINES VBP MAINSTREAM & SUBPOPULATIONS
II. Reporting Guidelines VBP Mainstream & Subpopulations
Mainstream & Subpopulation VBP Arrangements [Other than MLTC]
The State is requesting that Medicaid Managed Care (MMC) plans submit data files that leverage their 2021 QARR (HEDIS) submission which will be used to create aggregated quality results by VBP Contractor for all members in a VBP Arrangement. Specifically, the State is asking insurers to provide a modified version of the NYS Patient-Level Detail (PLD) file, along with provider and practice information. Submission of the NYS Patient Centered Medical Home (PCMH) Patient Level Detailed file for all members in a Level 1 or higher VBP Arrangement will fulfill this reporting requirement. The NYS PCMH Patient-Level Detail File layout is included in Section III of this manual. The State is also requesting a separate Patient Attribution file for all members in a Level 1 or higher VBP Arrangement. The Patient Attribution file layout is included in Section IV.
Table 1: 2021 VBP List of Required Measures
- Lists, by arrangement, the 2021 VBP Category 1 Measure sets and indicates the 2021 measures the State is requiring for reporting.
- Section IV: File Specifications required for reporting.
- This manual describes reporting requirements only. For VBP reporting or contracting questions, please contact OQPSVBP@health.ny.gov.
- Organizations must purchase the HEDIS® 2021/2022 Technical Specifications for descriptions of the required HEDIS® measures. For specifications for other non-HEDIS measures, please contact the measure steward for the correct version of the specification. NYS-specific measures are defined in the 2020-2021 Quality Assurance Reporting Requirements (QARR) Technical Specifications Manual.
MEASURE CHANGES
To maintain alignment with NCQA/HEDIS©'s1 shift in their timeline for publishing measure specifications, VBP measures were frozen for MY2020-2021. There were no additional measure changes to the VBP Reporting Requirements for MY2021. For a list of updates and changes for MY2020, you should refer to your 2021 VBP Reporting Requirements Technical Specifications Manual.
WHERE TO SUBMIT VBP REPORTING DATA
- Electronically submit all files (no later than 11:59 p.m. ET on Friday, July 29, 2022) via a secure file transfer facility. Do not mail materials.
- Specific delivery instructions are given for each file.
WHAT TO SEND FOR VBP REPORTING
- The State is requesting a NYS PCMH file and a Patient Attribution file for ALL members in a VBP Level 1 or higher Arrangement.
*****All submissions must be received electronically by 11:59 p.m. ET on Friday, July 29, 2022.*****
QUESTIONS CONCERNING 2022 VBP REPORTING
Please submit all questions to OQPSVBP@health.ny.gov.
___________________________
1. HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).
|top of section| |table of contents|III. Reporting Requirements
TABLE 1: 2022 VBP LIST OF REQUIRED MEASURES
| Measures | Notes | Arrangement Type | NQF ID | Specifications | Class | Children's | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| TCGP | IPC | Maternity | HARP | HIV/AIDS | ||||||
| Total Care for the General Population (TCGP)/ Integrated Primary Care (IPC) | ||||||||||
| Adherence to Antipsychotic Medications for Individuals with Schizophrenia (SAA) | ✓ | NA | NA | ✓ | NA | NA | 1879 | CMS 2018 | P4P | |
| Adherence to Mood Stabilizers for Individuals with Bipolar I Disorder | NR | NR | NA | NA | NR | NA | 1880 | HEDIS 2021/2022 | P4P | |
| Antidepressant Medication Management (AMM) | ✓ | ✓ | NA | NA | ✓ | NA | 105 | HEDIS 2021/2022 | P4P | |
| Asthma Admission Rate [PDI #14] (AMR) | NR | NR | NA | NA | NA | ✓ | 728 | AHRQ | P4P | |
| Asthma Medication Ratio (AMR) | ✓ | ✓ | NA | ✓ | ✓ | ✓ | 1800 | HEDIS 2021/2022 | P4P | |
| Breast Cancer Screening (BCS) | ✓ | ✓ | NA | ✓ | ✓ | NA | 2372 | HEDIS 2021/2022 | P4P | |
| Cervical Cancer Screening (CCS) | 2 | ✓ | ✓ | NA | ✓ | ✓ | NA | 32 | HEDIS 2021/2022 | P4P |
| Child and Adolescent Well-Care Visits (WCV) | ✓ | ✓ | NA | NA | NA | ✓ | HEDIS 2021/2022 | P4P | ||
| Childhood Immunization Status - combination 3 (CIS) | 2 | ✓ | ✓ | NA | NA | NA | ✓ | 38 | HEDIS 2021/2022 | P4P |
| Chlamydia Screening in Women (CHL) | ✓ | ✓ | NA | ✓ | NA | ✓ | 33 | HEDIS 2021/2022 | P4P | |
| Colorectal Cancer Screening (COL) | 2 | ✓ | ✓ | NA | ✓ | ✓ | NA | 34 | HEDIS 2021/2022 | P4P |
| Comprehensive Diabetes Care: Eye Exams (retinal) Performed (CDC) | 2 | ✓ | ✓ | NA | ✓ | ✓ | NA | 55 | HEDIS 2021/2022 | P4P |
| Comprehensive Diabetes Care: Hemoglobin A1c (HbA1c) Poor Control (>9.0%) (CDC) | 2 | ✓ | ✓ | NA | ✓ | ✓ | NA | 59 | HEDIS 2021/2022 | P4P |
| Controlling High Blood Pressure (CBP) | 2 | ✓ | ✓ | NA | ✓ | ✓ | NA | 18 | HEDIS 2021/2022 | P4P |
| Depression Remissionor Response for Adolescents and Adults (DRR) | ✓ | ✓ | NA | NA | ✓ | ✓ | HEDIS 2021/2022 | P4R | ||
| Diabetes Screening for People with Schizophrenia or Bipolar Disorder Using Antipsychotic Medications (SSD) | ✓ | ✓ | NA | ✓ | ✓ | NA | 1932 | HEDIS 2021/2022 | P4P | |
| Follow-Up After Emergency Department Visit for Alcohol and Other Drug Dependence (FUA) | ✓ | NA | NA | ✓ | NA | NA | 2605 | HEDIS 2021/2022 | ||
| Follow-Up After Emergency Department Visit for Mental Illness (FUM) | ✓ | NA | NA | ✓ | NA | NA | 3489 | HEDIS 2021/2022 | P4P | |
| Follow-Up After High-Intensity Care for Substance Use Disorder (FUI) | ✓ | NA | NA | ✓ | NA | NA | HEDIS 2021/2022 | |||
| Follow-Up After Hospitalization for Mental Illness (FUH) | ✓ | NA | NA | ✓ | NA | NA | 576 | HEDIS 2021/2022 | P4P | |
| HIV Viral Load Suppression (ASF) | 1 | ✓ | NA | NA | NA | ✓ | NA | 2082 | HRSA | P4P |
| Immunizations for Adolescents - Combination 2 (IMA) | ✓ | ✓ | NA | NA | NA | ✓ | 1407 | HEDIS 2021/2022 | P4P | |
| Initiation and Engagement of Alcohol & Other Drug Abuse or Dependence Treatment (IET) | ✓ | ✓ | ✓ | NA | ✓ | NA | 4 | HEDIS 2021/2022 | P4P | |
| Initiation of Pharmacotherapy upon New Episode of Opioid Dependence | ✓ | ✓ | NA | ✓ | ✓ | NA | NYS 2021/2022 | P4P | ||
| Kidney Health Evaluation for Patients With Diabetes (KED) | ✓ | ✓ | NA | ✓ | ✓ | NA | HEDIS 2021/2022 | P4P | ||
| Pharmacotherapy for Opioid Use Disorder (POD) | ✓ | NA | NA | ✓ | NA | NA | 3175 | NYS 2021/2022 | P4P | |
| Potentially Preventable Mental Health Related Readmission Rate 30 Days | ✓ | NA | NA | ✓ | NA | NA | NYS 2021/2022 | P4P | ||
| Prenatal and Postpartum Care (PPC) | ✓ | NA | ✓ | NA | NA | NA | 1517 Lost Endorsement | HEDIS 2021/2022 | P4P | |
| Well-Child Visits in the First 30 Months of Life (W30) | ✓ | ✓ | NA | NA | NA | ✓ | 1392 | HEDIS 2021/2022 | P4P | |
| Integrated Primary Care (IPC) | ||||||||||
| Adolescent Preventive Care Measures | 2 | NA | ✓ | NA | NA | NA | ✓ | NYS 2021/2022 | P4R | |
| Annual Dental Visit (ADV) | NA | ✓ | NA | NA | NA | ✓ | 1388 | HEDIS 2021/2022 | P4R | |
| Depression Screening and Follow-Up for Adolescents and Adults (DSF-E) | NA | NR | NR | NA | NR | NR | HEDIS 2021/2022 | P4R | ||
| Follow-Up Care for Children Prescribed ADHD Medication (ADD) | NA | ✓ | NA | NA | NA | ✓ | 108 | HEDIS 2021/2022 | P4R | |
| Potentially Avoidable Complications (PAC) in Routine Sick Care or Chronic Care | NA | NR | NA | NA | NA | NA | Altarum | P4R | ||
| Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan | NA | NR | NA | NR | NR | NA | 421 | CMS 2021 | P4R | |
| Preventive Care and Screening: Influenza Immunization | NA | ✓ | NA | ✓ | ✓ | NA | 41 | AMA PCPI | P4R | |
| Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention | NA | ✓ | ✓ | ✓ | ✓ | NA | 28 | AMA PCPI | P4R | |
| Statin Therapy for Patients with Cardiovascular Disease (SPC) | NA | ✓ | NA | ✓ | ✓ | NA | HEDIS 2021/2022 | P4R | ||
| Use of Pharmacotherapy for Alcohol Abuse or Dependence | NA | ✓ | NA | ✓ | ✓ | NA | NYS 2021/2022 | P4R | ||
| Use of Spirometry Testing in the Assessment and Diagnosis of COPD (SPR) | NA | ✓ | NA | ✓ | ✓ | NA | 577 | HEDIS 2021/2022 | P4R | |
| Weight Assessment and Counseling for Nutrition and Physical Activity for Children/Adolescents (WCC) | 2 | NA | ✓ | NA | NA | NA | ✓ | 24 | HEDIS 2021/2022 | P4P |
| Maternity | ||||||||||
| Contraceptive Care - Postpartum | NA | NA | NR | NA | NA | NA | 2902 | US Office of Population Affairs | P4R | |
| C-Section for Nulliparous Singleton Term Vertex (NSTV) (PC-02) | NA | NA | NR | NA | NA | NA | 471 | TJC 2019 | P4R | |
| Exclusively Breast Milk Feeding (PC-05) | NA | NA | NR | NA | NA | NA | 480 | TJC 2017 | P4R | |
| Incidence of Episiotomy | NA | NA | NR | NA | NA | NA | 470 | Christiana Care Health System 2019 | P4R | |
| Low Birth Weight [Live births weighing less than 2,500 grams (preterm v. full term)] | NA | NA | ✓ | NA | NA | NA | 278 Lost Endorsement | AHRQv7.0 | P4R | |
| Percentage of Preterm Births | NA | NA | NR | NA | NA | NA | NYS 2021 Vital Statics | P4R | ||
| Health and Recovery Program (HARP) | ||||||||||
| Completion of Home and Community Based Services Annual Needs Assessment | NA | NA | NA | ✓ | NA | NA | NYS 2021/2022 | P4R | ||
| Employed, Seeking Employment or Enrolled in a Formal Education Program | 1 | NA | NA | NA | ✓ | NA | NA | NYS 2021/2022 | P4R | |
| Stable Housing Status | 1 | NA | NA | NA | ✓ | NA | NA | NYS 2021/2022 | P4R | |
| No Arrests in the Past Year | 1 | NA | NA | NA | ✓ | NA | NA | NYS 2021/2022 | P4R | |
| Percentage of Members Enrolled in a Health Home | 1 | NA | NA | NA | NR | NA | NA | NYS 2021/2022 | P4R | |
| HIV/AIDS | ||||||||||
| Potentially Avoidable Complication (PAC) in Patients with HIV/AIDS | 1 | NA | NA | NA | NA | NR | Altarum | P4R | ||
| Sexually Transmitted Infections: Screening for Chlamydia, Gonorrhea, and Syphilis | 1 | NA | NA | NA | NA | ✓ | NYS 2021/2022 | P4P | ||
| CHILDREN | ||||||||||
| Developmental Screening Using Standardized Tool, First Three Years of Life | NA | NA | NA | NA | NR | 1488 Lost Endorsement | Oregon Health& Science University | P4R | ||
✓ - Required to Report NA - Not Applicable to the Arrangement Shading - Purple- Not required to be reported
1 - There are no reporting requirements for this measure. NYS will calculate the measure result for MY2021
2 - For measures that you may have reported using the hybrid sample in the PLD for QARR,
we request that you report the administrative denominator and numerator for VBP.
IV. File Specifications - Mainstream VBP
NYS PCMH Scorecard Patient-Level Detail File
Please use your 2021 QARR/HEDIS data warehouse as the source for this information. Do not recalculate or update measure results. However, in addition to the measure elements that you reported for QARR/HEDIS for 2021, we are requesting that you include the provider/practice that was attributed to the member using your own plan's attribution methodology for the IPC or TCGP arrangement. Several fields regarding the provider and practice site of the service have been added to the layout request for this purpose, specifically two separate fields for TIN: Practice TIN and Contractor TIN. In addition to Contractor TIN as health plans contract with different types of entities, such as providers, hospital systems, Independent Practice Associations (IPAs), and Accountable Care Organizations (ACOs) we have added a Contractor Type field. This information has been added to allow us to aggregate the results by VBP Contractor across all New York State MCOs.
The NYS PCMH data file is modeled after the NYS 2021 Patient-Level Detail file (PLD) that you prepared as part of your QARR submission, and many of the data elements in the NYS PCMH file follow the same definitions and format as used to define the data elements in the PLD. You may find it helpful to use the PLD as a resource or starting point in completing the NYS PCMH file.We ask that you populate the NYS PCMH with all Lines of Business that you serve , e.g., Medicaid. Once completed, please upload the file to IPRO's FTP site. A subfolder in the "QARR 2022" folder where you will upload your 2021 QARR files entitled "NYS PCMH 2022" will be created for your submission. If someone other than your QARR liaison will be responsible for NYS PCMH reporting, please contact the VBP Team at the email address below for access to the FTP site. Please note that the deadline for submission is Friday, July 29, 2022.
Exceptions to the PLD file are noted below:
- The NYS PCMH file requests Medicare HEDIS data, which is not required for QARR reporting.
- The Plan ID is not your plan's QARR ID. The Plan ID field should be populated with the Organization ID that you used to submit the IDSS to NCQA.
- Note that the Organization ID is different from the Submission ID. Submission ID which is specific to a Line of Business.
- The Organization ID provides six digits. If your plan's ID is smaller, please right justify.
- For Medicaid, we ask that you populate the Member's CIN in the ID field.
- The field is alphanumeric and should be treated as a text field. This field is mandatory - do not leave it blank!
- Provider/Practice attribution information is required for NYS PCMH. This information is not required for QARR reporting.
Specific Instructions:
- If a member is reported for a specific measure in more than one product line (e.g., duals), please report them for only one product, using the following priority: Commercial, then Medicare, then Medicaid. This instruction affects only members who may be reported twice for the same service.
- A Unique Member ID may be included on the file more than once if the member is in more than one product line during the reporting period.
- For measures that you may have reported using the hybrid sample in the NYS PLD, we request that you report the administrative denominator and numerator from the IDSS for NYS PCMH.
- Members in the file must be in at least one measure.
- Measures that do not apply to the member should be zero-filled.
- A valid Tax ID (TIN) is nine characters. If the TIN is not available, set the field value to "999999999."
- Practice Name must be populated in the Practice Name only.
- Practice Address Line 1 must contain the street address of the Practice, not the Practice Name.
- For Fields #7-22, leave these fields blank if the member cannot be attributed to any provider and you are not able to identify the provider.
- For Field # 21, Populate with valid TINs only. If the member is NOT attributed to a VBP Contractor set to '999999999'.
- The IET Engagement numerator value must be less than or equal to the Initiation numerator (Field #87 and 90) value.
- For the AAB (Field #83) and LBP measures, provide the actual numerator (non-inverted), e.g., for AAB, the numerator would be members receiving the antibiotic.
- For the AMB measure, please populate the fields with the number of events for each LOB you are reporting. Member Months are not required for 2022.
- For the IPU/AHU/EDU measures, please populate the fields with the number of events for each LOB you are reporting. Member Months are not required for 2022.
- Only MCOs reporting their Medicaid line of Business need to report the following 8 VBP specific measures: Statin Therapy for Patients with Cardiovascular Disease, Use of Spirometry Testing in the Assessment and Diagnosis of COPD, Diabetes Screening for Schizophrenia or Bipolar Disorder Who Are Using Antipsychotic Medications, Initiation of Pharmacotherapy Upon New Episode of Opioid Dependence, Weight Assessment and Counseling for Nutrition and Physical Activity for Children/Adolescents (Administrative rate), Follow-Up Care for Children Prescribed ADHD Medication, Annual Dental Visit, Well-Child Visits in the First 30 Months of Life. Medicaid plans submitting NYS PCMH data should add these additional variables to the NYS PCMH file layout, and it will count towards the VBP reporting requirements.
For questions regarding this request, please contact the VBP Team of OQPS at: OQPSVBP@health.ny.gov or (518) 486-9012. The NYS PCMH Patient-Level Detail File Layout was released in March of 2021. The specifications/file layout for the PCMH file for this year is the same as those released in March 2021.
Patient Attribution File
The State is asking insurers to provide an attribution file for all members enrolled in a VBP arrangement during the 2021 Calendar Year per the methodology specified in your state-approved contract. The attribution file will be used in combination with other quality measure sources (e.g., 2022 NYS Patient-Level Detail File) to aggregate quality results for the 2021 Category 1 population-specific measures by VBP Contractor.
NOTE: MLTC attribution instructions are different than for other populations. Please follow the instructions in the MLTC attribution file subsection of this manual.
File Format:
Submit a text file that is either: fixed-width (TXT) or comma-separated values (CSV)
Fixed-width TXT files:
- Must have column start/end locations as documented in the following table.
- Data must not include column names. The first row in the file must be data.
- Numeric values should be right justified, and blank filled to the left of the value; text fields should be left-justified, and blank filled to the right of the value. Variable character (VARCHAR) fields should be treated as text.
CSV files:
- Must not have additional columns beyond those shown in the following table. (Refer to companion excel file.)
- Data must include column names. The first row in the file must be the column names as documented in the following table.
Naming Convention:
The file should be named VBP_PlanID_2021.txt or VBP_PlanID_2021.cvs (Refer to field 1 in table below.)

All files are due no later than Friday, July 29, 2022.
| Element # | Name | Direction | Allowed Values | Data Type | Required/Optional | Length | Start | End |
|---|---|---|---|---|---|---|---|---|
| 1 | Plan_ID# | Organization ID used to submit the IDSS to NCQA. This ID is consistent across all Lines of Business. | ###### | VARCHAR | R | 6 | 1 | 6 |
| 2 | Product_Line | A member's product line at the end of the measurement period. | 1 = MEDICAID 2 = SNP 11 = HARP | NUMBER | R | 2 | 7 | 8 |
| 3 | Unique_Member_ ID# | Medicaid Client ID Number (CIN) *The field is alphanumeric and should be treated as a text field. This field is mandatory - do not leave it blank! | VARCHAR | R | 8 | 9 | 16 | |
| 4 | County_of_ Residence | Enter the 3-digit county FIPS code for each member's county of residence. | ### | NUMBER | R | 3 | 17 | 19 |
| 5 | Zip_Code_of_ Residence | ##### | NUMBER | R | 5 | 20 | 24 | |
| 6 | Practice_Tax_ID# | Populate with valid TINs only. This field is mandatory - do not leave it blank! | ######### | NUMBER | R | 9 | 25 | 33 |
| 7 | PCMH_Site_ID# | PCMH Site ID# - NCQA generated ID | NUMBER | O | 11 | 34 | 44 | |
| 8 | Practice_Site_ID# | Internal plan practice site ID# | VARCHAR | O | 13 | 45 | 57 | |
| 9 | Practice_Name | This field is mandatory - do not leave it blank! | TEXT | R | 50 | 58 | 107 | |
| 10 | Practice_Address_ Line_1 | TEXT | R | 35 | 108 | 142 | ||
| 11 | Practice_Address_ Line_2 | TEXT | O | 35 | 143 | 177 | ||
| 12 | Practice_Address_ Line_3 | TEXT | O | 35 | 178 | 212 | ||
| 13 | Practice_Address_ City | TEXT | R | 25 | 213 | 237 | ||
| 14 | Practice_Address_ State | TEXT | R | 2 | 238 | 239 | ||
| 15 | Practice_Address_ Zip_Code | ##### | NUMBER | R | 5 | 240 | 244 | |
| 16 | Practice_Telephone _Number | ########## | NUMBER | O | 10 | 245 | 254 | |
| 17 | Provider_NPI | National Provider Identifier - 10 Digit ID | ########## | NUMBER | R | 10 | 255 | 264 |
| 18 | Provider_First_ Name | TEXT | R | 15 | 265 | 279 | ||
| 19 | Provider_Middle_ Initial | TEXT | O | 1 | 280 | 280 | ||
| 20 | Provider_Last_ Name | TEXT | R | 35 | 281 | 315 | ||
| 21 | VBP_Contractor_ Tax_ID# | Populate with valid TINs only. Please include the TIN of the VBP Contractor (not the provider) If the member is NOT in a VBP level 1 or higher arrangement set to '999999999'. | ######### | NUMBER | R | 9 | 316 | 324 |
| 22 | VBP_Contractor_ DBA_Name | Enter the DBA name listed on your VBP contract/arrangement. | VARCHAR | R | 50 | 325 | 374 | |
| 23 | VBP_Contractor_ Type | 1 = Provider/ Hospital 2 = IPA 3 = ACO 9 = Unknown | NUMBER | R | 1 | 375 | 375 | |
| 24 | VBP_Arrangement_ Type | Refer to Section C, #2b of the DOH 4255 - Provider Contract Statement and Certification form. | 1 = TCGP 2 = IPC 3 = HARP 4 = HIV/AIDs 5 = Maternity 6 = Off Menu | NUMBER | R | 1 | 376 | 376 |
| 25 * | DOH_VBP_Contract _ID# | The number provided by DOH in the Agreement approval letter begins with DOH ID ### | #### | NUMBER | R | 4 | 377 | 380 |
| 26 * | MCO_Unique_ Contract_ID# | Plan generated ID used to submit contract to DOH; Section A, #3 of the 4255. | VARCHAR | R | 50 | 381 | 430 | |
| 27 | Prov_Att_start_date | MMDDYYYY - Must be between 1/1/2021 and 12/31/2021 | MMDDYYYY | DATE | R | 8 | 431 | 438 |
| 28 | Prov_Att_end_date | MMDDYYYY - Must be between 1/1/2021 and 12/31/2021 | MMDDYYYY | DATE | R | 8 | 439 | 446 |
| Field | Field Name | Description/Specifications |
|---|---|---|
| 1 | Plan_ID# | Enter your Organization ID used to submit the IDSS to NCQA. This ID is consistent across all Lines of Business. |
| 2 | Product_Line | Enter the member's product line at the end of the measurement period. Enter the corresponding number (1) Medicaid, (2) SNP, (11) HARP. |
| 3 | Unique_Member_ID# | Enter member's Medicaid Client Identification Number (CIN). The field should be continuous without any spaces or hyphens. The field is alpha-numeric and should be treated as a text field. This field is mandatory- do not leave it blank! |
| 4 | County_of_Residence | Enter the Federal Information Processing Standard (FIPS) code for the member's county of residence. Please refer to Appendix IV, Table 5 - NYS FIPS Codes by County at the end of this manual for a complete listing of NYS FIPS codes. |
| 5 | Zip_Code_of_Residence | Enter the 5-digit zip code of the member's residence. |
| 6 | Practice_Tax_ID# | Enter the 9-digit Federally assigned Tax Identification Number for the Practice of the member's provider. Populate with valid TINs only. This field is mandatory - do not leave it blank! |
| 7 | PCMH_Site_ID# | Enter the NCQA assigned number associated with your Patient-Centered Medical Home (PCHM.) |
| 8 | Practice_Site_ID# | Enter your internal site ID assigned by the plan. |
| 9 | Practice_Name | Enter the complete name of the provider's practice. This field is required, do not leave blank. |
| 10 11 12 | Practice_Address_Line_1 Practice_Address_Line_2 Practice_Address_Line_3 | Enter the physical address of the practice location. (Enter up to 3 lines) |
| 13 | Practice_Address_City | Enter the city in which the practice is located. |
| 14 | Practice_Address_State | Enter the 2-digit abbreviation for the state in which the practice is located. |
| 15 | Practice_Address_Zip_Code | Enter the 5-digit zip code in which the practice is located. |
| 16 | Practice_Telephone_Number | Enter the practice's main phone line, it should be in the format of ########## with no intervening "-". |
| 17 | Provider_NPI | This is the unique 10-digit National Provider Identifier (NPI) of the provider the member was serviced by during the reporting period. This should be a provider organization that had frequent contact with the member and, therefore, could potentially affect the need for hospitalization or not. A member may be serviced by multiple providers during the same time period (provide one row of data for every provider a member was serviced by). |
| 18 | Provider_First_Name | Enter the provider full first name |
| 19 | Provider_Middle_Initial | Enter the provider's middle initial. |
| 20 | Provider_Last_Name | Enter the provider's last name. |
| 21 | VBP_Contractor_Tax_ID# | This is the unique 9-digit tax identification number of the VBP Contractor (not the provider) that the member is assigned to a Level 1 or higher VBP arrangement during the reporting period. A member can only be assigned to one VBP contractor at a time. If not applicable, fill with 999999999. |
| 22 | VBP_Contractor_DBA_Name | The "Doing Business As" (DBA) name is the operating name of a company, as opposed to the legal name of the company. The VBP Contractor may be an ACO, IPA, individual provider, or hospital. |
| 23 | VBP_Contractor_Type | In this field, enter '1' if the contractor is a provider (provider includes hospitals), '2' if the contractor is an IPA, '3' if the contractor is an ACO, '9' if Unknown |
| 24 | VBP_Arrangement_Type | In this field, enter "1" if the VBP arrangement type is a TCGP arrangement, "2" if it is an IPC arrangement, "3" if it is a HARP arrangement, "4" if it is an HIV/AIDs arrangement, "5" if it is a Maternity arrangement, "6" if it is an Off-Menu arrangement. This information can be found in Section C, #2b of the DOH 4255 - Provider Contract Statement and Certification form. |
| 25 * | DOH_VBP_Contract_ID# | This is the number provided by DOH in the Agreement approval letter for your VBP arrangement, it begins with DOH ID ####. * You must populate either field 25 or 26, preferably both fields should be populated. If you need assistance obtaining your correct DOH VBP Contract Identifier, please email NYS DOH VBP mailbox at OQPSVBP@health.ny.gov |
| 26 * | MCO_Unique_Contract_ID# | This is the contract identifier created by your plan, which is a required component of all contracts submitted for review (it can be found in Section A, #3 of the DOH 4255, it is also typically in the footer of your contract documents. * You must populate either field 25 or 26, preferably both fields should be populated. If you need assistance obtaining your correct MCO Unique Contract Identifier, please email NYS DOH VBP mailbox at OQPSVBP@health.ny.gov |
| 27 | Prov_Att_start_date | This is the attribution start date with the provider when the member was first attributed to the provider. This date must be during the reporting period. It should be in the format of MMDDYYYY with no intervening "-" or "/". The format is the same if data is submitted via a fixed-width file or CSV. |
| 28 | Prov_Att_end_date | This is the attribution end date with the provider when the member was last attributed to the provider. This date must be during the reporting period. It should be in the format of MMDDYYYY with no intervening "-" or "/". The format is the same if data is submitted via a fixed-width file or CSV. |
Submission Examples and Data Requirements Checklist
Please refer to section VIII Appendix, Table 6 at the end of this manual, for layout examples of both TXT and CSV files.
Please refer to section VIII Appendix, Table 7 at the end of this manual, for attribution file checklists for the MCO attribution file. The checklist is designed to ensure fields in the attribution file are standardized appropriately and are not required to be submitted with the attribution files.
File Submission:
Files for all arrangement types are to be submitted to the New York State Department of Health via the Secure File Transfer 2.0 of the Health Commerce System (HCS). Files should be submitted to OQPS VBP Evaluation or OQPSVBP@health.ny.gov via HCS.
Files must be submitted by close of business on Friday, July 29, 2022.
|top of section| |table of contents|REPORTING GUIDELINES VBP MLTC
V. Reporting Guidelines VBP MLTC
The State is requesting insurers to submit a Patient Attribution file, which will be used to create aggregated quality results by Provider or VBP Contractor. DOH will calculate all reportable Category 1 quality measure results for the arrangements. The attribution methodology and Patient Attribution file layout are included in Section VI of this document.
- Table 2: 2022 MLTC VBP List of Required Measures
- Lists, by arrangement, the 2022 MLTC VBP Category 1 Measure set and indicates the 2022 measures required for reporting.
Measure Changes
Changes to the Reporting Requirements for 2022 Measure Sets were made based on the feedback received by the DOH from the Clinical Advisory Groups, Measure Support Task Force and Sub-teams, and from other stakeholder groups. Those changes are indicated below. In instances where a measure was moved from Category 1 in MY2021 to Category 2 in MY2022 or removed entirely, the State will not require reporting of the data related to those measures.
MLTC:
Category 1: Change
- Kidney Health Evaluation for Patients with Diabetes (KED); added as a MAP Required (P4R) Category 1 Measure added as a MAP Required Category 1 Measure
Category 2: Change
- All measures based on MDS 3.0 (the Centers for Medicare and Medicaid Services Minimum Data Set for nursing home members) have been removed from the MLTC measure set.
Table 2: 2022 MLTC VBP List of Required Measures
| Measures | Notes | Arrangement Type | NQF ID | Specifications | Class |
|---|---|---|---|---|---|
| MLTC | |||||
| Managed Long-Term Care (MLTC) | |||||
| Percentage of members who did not have an emergency room visit in the last 90 days | 1 | ✓ | NYS 2022 | P4P | |
| Percentage of members who did not experience falls that resulted in major or minor injury in the last 90 days | 1 | ✓ | NYS 2022 | P4P | |
| Percentage of members who received an influenza vaccination in the last year | 1 | ✓ | NYS 2022 | P4P | |
| Percentage of members who did not experience uncontrolled pain | 1 | ✓ | NYS 2022 | P4P | |
| Percentage of members who were not lonely or were not distressed | 1 | ✓ | NYS 2022 | P4P | |
| Potentially Avoidable Hospitalizations (PAH) for a primary diagnosis of heart failure, respiratory infection, electrolyte imbalance, sepsis, anemia, or urinary tract infection | 1, 2 | ✓ | NYS 2022 | P4P | |
✓ - Required to Report NA - Not Applicable to the Arrangement Shading - Purple- Not required to be reported
1 - There are no reporting requirements for this measure. NYS will calculate the measure result for MY2021/2022
2 - NYS will calculate this measure for the community-based providers.
VI. File Specifications - VBP MLTC
MLTC Attribution File
For 2022, all P4P Category 1 measures for the MLTC arrangement will be computed by DOH to reduce the burden on the MTLC plans. With the Public Health Emergency due to COVID, Community Health Assessment (CHA) based measure calculation will be dependent on the impact of reassessment mortarium.
Attribution Methodology:
MAP/PACE: Plan enrollees who have four or more months of continuous enrollment from April 2021 through June 2022 should be submitted in this attribution file. This attribution should be to provider organizations of CHHA, LHCSA, and, VBP contractor (if applicable) which had the most frequent contact with the member and, therefore, could potentially affect quality measures. Services being received by the member through Consumer Directed Personal Assistance (CDPAS) should not be included in this attribution file.
Changes to the NYS Long-Term Care VBP Initiative for 2022: MLTC Partial plans have been phased out of VBP as a result of the enacted SFY 2021-21 Budget. Plans are encouraged to continue to submit VBP arrangements for MAP and PACE consistent with standards outlined in the VBP Roadmap and the Provider Contract Guidelines for Article 44 MCOs, IPAs, and ACOs. Please note, MLTC Partial plans are not required to submit VBP attribution data beginning in 2022.
File Format:
- Include only members who had 4 months or more continuous enrollment in an MLTC plan from April 2021 through June 2022.
- For each member from step 1, list all provider organization(s) that provided at least one service per month, for 4 or more continuous months from April 2021 through June 2022. The data should be formatted in a long form containing one row of data for each member/provider combination. Please provide at least one row of data for every provider a member was serviced by (see Examples 1 and 2 below). If a member does not have any providers from which they received 4 or more continuous months of care, THE MEMBER SHOULD NOT BE LISTED.
- The text file must be either: 1) fixed width and named PROVIDERS_MLTC.TXT, or 2) comma-separated values (CSV) and named PROVIDERS_MLTC.CSV.
- Fixed-width files
- Must have column start/end locations as documented in the following table.
- Data must not include column names. The first row in the file must be data.
- CSV files
- Must not have additional columns beyond those shown in the following table.
- Data must include column names. The first row in the file must be the column names as documented in the following table.
- Fixed-width files
- The following table provides instructions on the submission of member-level data.
# Field Name Data Type Length Start Colum End Column Details/Comments 1 CIN Varchar 8 1 8 A Participant's Medicaid client identification number. The field should be continuous without any spaces or hyphens. The field is alpha-numeric and should be treated as a text field. This field may not be NULL 2 MMIS_ID Varchar 8 9 16 The MLTC Plan's numeric eight-digit ID. This field may not be NULL. 3 Prov_NPI Varchar 10 17 26 The unique 10-digit National Provider Identifier (NPI) for the provider the member was serviced by during the reporting period. 4 Prov_start_ date Date 8 27 34 MMDDYYYY - Must be between April 2021 - June 2022 5 Prov_end_date Date 8 35 42 MMDDYYYY - Must be between April 2021 - June 2022 6 Contractor_TIN Varchar 9 43 51 The unique 9-digit tax identification number of the VBP Contractor. Only submit the TIN, if this member is included in a level 2 or higher arrangement with a VBP Contractor. If not applicable or level 1 arrangement, fill with 999999999. 7 Contractor_Type Varchar 1 52 52 1= CHHA, LHCSA, 2= IPA, 3= Hospital, 4= ACO, 8= Other, and 9 = NA. Only submit if this member is included in a level 2 or higher arrangement with a VBP Contractor. If not applicable or level 1 arrangement, fill 9 = NA. 8* DOH_VBP_ Contract_# Number 4 53 56 The number provided by DOH in the Agreement approval letter begins with DOH ID ###. You must populate either field 8 or 9, preferably both fields should be populated. 9* MCO_Unique_ Contract_ID# Varchar 50 57 107 Plan generated ID used to submit contract to DOH; Section A, #3 of the 4255. You must populate either field 8 or 9, preferably both.
Field Definitions:
Prov_NPI: This is the unique 10-digit National Provider Identifier (NPI) of the provider the member was serviced by during the reporting period. This should be a provider organization that had frequent contact with the member and, therefore, could potentially affect the need for hospitalization or not. A member may be serviced by multiple providers during the same time period (provide one row of data for every provider a member was serviced by).
Prov_start_date: This is the service start date with the provider. This date must be during the reporting period. It should be in the format of MMDDYYYY with no intervening "-" or "/". The format is the same if data is submitted via a fixed-width file or CSV.
Prov_end_date: This is the service end date with the provider. This date must be during the reporting period. It should be in the format of MMDDYYYY with no intervening "-" or "/". The format is the same if data is submitted via a fixed-width file or CSV.
Contractor TIN: This is the unique 9-digit tax identification number of the VBP Contractor (not the provider) that the member is assigned to for a Level 2 arrangement during the reporting period. A member can only be assigned to one level 2 or higher VBP contractor at a time. If not applicable or level 1, fill with 999999999.
Contractor_Type: The VBP Contractor may be an ACO, IPA, hospital, or large LHCSA/CHHA that is coordinating services for many LHCSAs or CHHAs. This field is for the VBP Contractor (not the provider) that the member is assigned to a level 2 or higher arrangement during the reporting period. A member can only be assigned to one level 2 or higher VBP contractor at a time. If not applicable or level 1 arrangement, fill with 9.
* DOH_VBP_Contract_#: This is the number provided by DOH in the Agreement approval letter for your VBP arrangement, it begins with DOH ID ####.
* MCO_Unique_Contract_ID#: This is the contract identifier created by your plan, which is a required component of all contracts submitted for review (it can be found in Section A, #3 of the DOH 4255, it is also typically in the footer of your contract documents.
Data Requirements Checklist
Please refer to section VIII Appendix, Table 8 at the end of this manual, for attribution file checklists for the MLTC attribution file. The checklist is designed to ensure fields in the attribution file are standardized appropriately and are not required to be submitted with the attribution files.
File Submission:
Files are to be submitted to the New York State Department of Health via the Secure File Transfer 2.0 of the Health Commerce System. Files should be submitted to OQPS MLTC Evaluation mailbox. Files are to be submitted by close of business on Friday, July 29, 2022.
NOTE: When a Provider/NPI has overlapping service dates for a member, the service dates should be collapsed into one record with the earliest start date and furthest end date. Multiple rows for the same member/provider may be provided only if the provider/NPI has nonoverlapping service dates and each time frame meets the 4 months of service criterion. (see Example 3 below).
Submission Examples:
Example 1 and 2 below illustrates two different providers, with overlapping services dates, adding a single member from February through June 2022.
Example 1 below illustrates a member who was continuously enrolled for 4 or more months in the health plan and received at least one service per month from same provider organization for 4 or more continuous months, for two separate non-overlapping time periods and is covered by level 2 or higher VBP contract during April 2021 through June 2022.
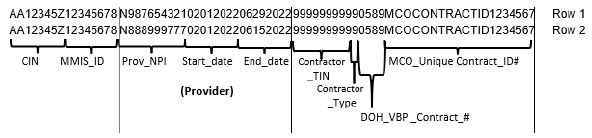
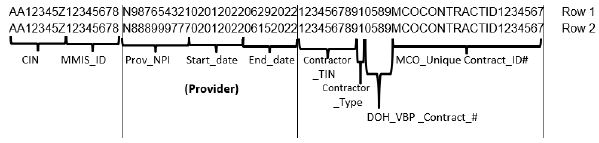
Example 2
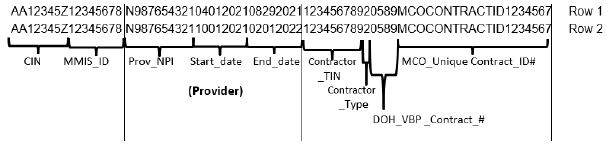
Example 3 below illustrates a member who was continuously enrolled for 4 or more months in the health plan and received at least one service per month from same provider organization for 4 or more continuous months, for two separate non-overlapping time periods and is covered by level 2 or higher VBP contract during April 2021 through June 2022.
Fully Capitated Plans:
Because the HEDIS and CMS-based P4R category 1 measures cannot be calculated by the State, plans must calculate and report Plan/Provider-VBP Contractor performance to the State by July 22, 2022. Files are to be submitted to the New York State Department of Health via the Secure File Transfer 2.0 of the Health Commerce System. Files should be submitted to the OQPS MLTC Evaluation mailbox.
Plans should submit an Excel file with the following format. Submit a row for each measure being reported. Plans are required to report on all measures for each plan-provider combination.
| # | Field Name * | Data Type | Excel Column Placement | Details/Comments |
|---|---|---|---|---|
| 1 | MMIS_ID | Varchar | Column A | The MLTC Plan's numeric eight-digit ID. This field may not be NULL. |
| 2 | Prov_NPI | Varchar | Column B | The unique 10-digit National Provider Identifier (NPI) for the provider the member was serviced by during the reporting period. This field may not be NULL. |
| 3 | Measure ID | Varchar | Column C | Use the measure ID from the table below |
| 4 | Denominator for Measure | Varchar | Column D | Report the total number of members included in the denominator for the given measure |
| 5 | Numerator for Measure | Varchar | Column E | Report the total number of members that were included in the numerator for the given measure |
| 6 | Exclusions for Measure | Varchar | Column F | Report the number of members excluded from the given measure |
| 7 | Rate for Measure | Varchar | Column G | Report the rate to the hundredth decimal place |
| 8 | Contractor_TIN | Varchar | Column H | The unique 9-digit tax identification number of the VBP Contractor. Only submit the TIN, if this member is included in a level 2 or higher arrangement with a VBP Contractor. If not applicable or level 1 arrangement, fill with 999999999. |
| 9 | Contractor_Type | Varchar | Column I | 1= CHHA, LHCSA, 2= IPA, 3= Hospital, 4= ACO, 8= Other, and 9= NA. Only submit if this member is included in a level 2 or higher arrangement with a VBP Contractor. If not applicable or level 1 arrangement, fill 9 = NA. |
| 10 * | DOH_VBP_ Contract_# | Varchar | Column J | The number provided by DOH in the Agreement approval letter begins with DOH ID ####. *You must populate either field 10 or 11, preferably both. |
| 11 * | MCO_Unique_ Contract_ID# | Varchar | Column K | Plan generated ID used to submit the contract to DOH; Section A, #3 of the 4255. *You must populate either field 10 or 11, preferably both. |
| * See Field Definitions under preceding MLTC Attribution File specifications | ||||
| Measure Name | Measure ID |
|---|---|
| MAP P4R measures (Measure Source/ Steward: NCQA/ HEDIS) | |
| Antidepressant Medication Management - Effective Acute Phase Treatment* | 1 |
| Antidepressant Medication Management - Effective Continuation Phase Treatment* | 2 |
| Colorectal Cancer Screening* | 3 |
| Eye Exam for Patients with Diabetes*,1 | 4 |
| Kidney Health Evaluation for Patients with Diabetes (KED)* | 5 |
| Follow-up After Hospitalization for Mental Illness - 7 Days^ | 6 |
| Follow-up After Hospitalization for Mental Illness - 30 Days^ | 7 |
| Initiation of Substance Use Disorder Treatment*,2 | 8 |
| Engagement of Substance Use Disorder Treatment*,2 | 9 |
| PACE P4R measures (Measure Source/ Steward: CMS) | |
| PACE Participant Emergency Department Utilization Without Hospitalization | 10 |
| Percentage of Participants Not in Nursing Homes | 11 |
| Percentage of Participants with an Annual Review of Their Advance Directive or Surrogate Decision-Maker AND Percentage of Participants With an Annual Review of Their Advance Directive or Surrogate Decision-Maker | 12 |
| * Included in the IPC/TCGP measure set ^ Included in the Health and Recovery Plan (HARP) measure set 1. Replacement HEDIS measure 2. Measure specifications/name revised by NCQA/NYS for 2022 HEDIS Measure set |
|
VII. APPENDIX
TABLE 3: 2022 MAINSTREAM VBP LIST OF CATEGORY 2 MEASURES
| Measures | Notes | Arrangement Type | NQF ID | Measure Steward | |||||
|---|---|---|---|---|---|---|---|---|---|
| TCGP | IPC | Maternity | HARP | HIV/AIDS | Children | ||||
| Integrated Primary Care (IPC) | |||||||||
| Asthma Action Plan | NA | Cat 2 | NA | Cat 2 | Cat 2 | NA | AAAAI | ||
| Asthma: Assessment of Asthma Control - Ambulatory Care Setting | NA | Cat 2 | NA | Cat 2 | Cat 2 | NA | AAAAI | ||
| Asthma: Lung Function/Spirometry Evaluation | NA | Cat 2 | NA | Cat 2 | Cat 2 | NA | AAAAI | ||
| Developmental Screening Using Standardized Tool, First Three Years of Life | NA | Cat 2 | NA | NA | NA | Cat 1 | 1488 | Oregon Health and Science University | |
| Follow-up after Emergency Department Visit For Mental Illness | Cat 1 | Cat 2 | NA | NA | NA | NA | 2605 | HEDIS 2021 | |
| Follow-Up After High-Intensity Care for Substance Use Disorder | Cat 1 | Cat 2 | NA | Cat 1 | NA | NA | NA | ||
| Home Management Plan of Care (HMPC) Document Given to Patient/Caregiver (asthma) | NA | Cat 2 | NA | Cat 2 | NA | 338 | The Joint Commission | ||
| Maternal Depression Screening | NA | Cat 2 | NA | NA | NA | Cat 2 | 1401 | HEDIS 20221 | |
| Screening for Reduced Visual Acuity and Referral in Children | NA | Cat 2 | NA | NA | NA | Cat 2 | 2721 | CMS | |
| Topical Fluoride for Children at Elevated Caries Risk, Dental Services | NA | Cat 2 | NA | Cat 2 | Cat 2 | Cat 2 | 2528 | American Dental Association | |
| Use of First-Line Psychosocial Care for Children and Adolescents on Antipsychotics | NA | Cat 2 | NA | NA | NA | Cat 2 | 2801 | HEDIS 2021 | |
| Use of Pharmacotherapy for Opioid Dependence | NA | Cat 2 | NA | Cat 2 | Cat 2 | NYS 2021 | |||
| Maternity | |||||||||
| Antenatal Steroids | NA | NA | Cat 2 | NA | NA | NA | 476 | TJC | |
| Appropriate DVT Prophylaxis in Women Undergoing Cesarean Delivery | NA | NA | Cat 2 | NA | NA | NA | 473 | Hospital Corporation of America | |
| Experience of Mother with Pregnancy Care | NA | NA | Cat 2 | NA | NA | NA | TBD | ||
| Hepatitis B Vaccine Coverage Among All Live Newborn Infants Prior to Hospital or Birthing Facility Discharge | NA | NA | Cat 2 | NA | NA | NA | 475 | Centers for Disease Control and Prevention | |
| Intrapartum Antibiotic Prophylaxis for Group B Streptococcus (GBS) | NA | NA | Cat 2 | NA | NA | NA | 1746 | Massachusetts General Hospital | |
| Prenatal Depression Screening and Follow-Up | NA | NA | Cat 2 | NA | NA | NA | NCQA | ||
| Postpartum Blood Pressure Monitoring | NA | NA | Cat 2 | NA | NA | NA | TBD | ||
| Vaginal Birth After Cesarean (VBAC) Delivery Rate, Uncomplicated | NA | NA | Cat 2 | NA | NA | NA | NYS 2021 | ||
| Health and Recovery Program (HARP) | |||||||||
| Adherence to Mood Stabilizers for Individuals with Bipolar I Disorder | NA | NA | NA | Cat 2 | NA | NA | 1880 | CMS | |
| Mental Health Engagement in Care - 30 Days | NA | NA | NA | Cat 2 | NA | NA | NYS 2021 | ||
| Percentage of HARP Enrolled Members Who Received Personalized Recovery Oriented Services (PROS) or Home and Community Based Services (HCBS) | NA | NA | NA | Cat 2 | NA | NA | NYS 2021 | ||
| HIV/AIDS | |||||||||
| Diabetes Screening | NA | NA | NA | NA | Cat 2 | NA | NYS DOH AIDS Institute | ||
| Hepatitis C Screening | NA | NA | NA | NA | Cat 2 | NA | HRSA | ||
| Housing Status | NA | NA | NA | NA | Cat 2 | NA | HRSA | ||
| Linkage to HIV Medical Care | NA | NA | NA | NA | Cat 2 | NA | NYS 2021 | ||
| Medical Case Management: Care Plan | NA | NA | NA | NA | Cat 2 | NA | HRSA | ||
| Prescription of HIV Antiretroviral Therapy | NA | NA | NA | NA | Cat 2 | NA | HRSA | ||
| Sexual History Taking: Anal, Oral, and Genital | NA | NA | NA | NA | Cat 2 | NA | NYS DOH AIDS Institute | ||
| Substance Abuse Screening | NA | NA | NA | NA | Cat 2 | NA | HRSA | ||
TABLE 4. 2022 VBP MLTC CATEGORY 2 MEASURES
| Measures | Notes | Arrangement Type | Measure source/Steward |
|---|---|---|---|
| MLTC | |||
| Care for Older Adults - Medication Review | Cat 2 | NCQA | |
| Use of High-Risk Medications in the Elderly | Cat 2 | NCQA | |
| Percentage of members who rated the quality of home health aide or personal care aide services within the last 6 months as good or excellent | 1 | Cat 2 | MLTC Survey/New York State |
| Percentage of members who responded that they were usually or always involved in making decisions about their plan of care | 1 | Cat 2 | MLTC Survey/New York State |
| Percentage of members who reported that within the last 6 months the home health aide or personal care aide services were always or usually on time | 1 | Cat 2 | MLTC Survey/New York State |
- Included in the NYS DOH MLTC Quality Incentive measure set
TABLE 5 - NYS FIPS CODES BY COUNTY
| County Name | FIPS Code | County Name | FIPS Code | County Name | FIPS Code |
|---|---|---|---|---|---|
| Albany | 001 | Jefferson | 045 | Schenectady | 093 |
| Allegany | 003 | Kings | 047 | Saratoga | 091 |
| Bronx | 005 | Lewis | 049 | Schoharie | 095 |
| Broome | 007 | Livingston | 051 | Schuyler | 097 |
| Cattaraugus | 009 | Madison | 053 | Seneca | 099 |
| Cayuga | 011 | Monroe | 055 | St. Lawrence | 089 |
| Chautauqua | 013 | Montgomery | 057 | Steuben | 101 |
| Chemung | 015 | Nassau | 059 | Suffolk | 103 |
| Chenango | 017 | New York | 061 | Sullivan | 105 |
| Clinton | 019 | Niagara | 063 | Tioga | 107 |
| Columbia | 021 | Oneida | 065 | Tompkins | 109 |
| Cortland | 023 | Onondaga | 067 | Ulster | 111 |
| Delaware | 025 | Ontario | 069 | Warren | 113 |
| Dutchess | 027 | Orange | 071 | Washington | 115 |
| Erie | 029 | Oswego | 075 | Wayne | 117 |
| Essex | 031 | Orleans | 073 | Westchester | 119 |
| Franklin | 033 | Otsego | 077 | Wyoming | 121 |
| Fulton | 035 | Putnam | 079 | Yates | 123 |
| Genesee | 037 | Queens | 081 | Out of State | 000 |
| Greene | 039 | Rensselaer | 083 | Unknown/Missing | 999 |
| Hamilton | 041 | Rockland | 087 | ||
| Herkimer | 043 | Richmond | 085 |
TABLE 6: SUBMISSION EXAMPLES
The example below illustrates one member attributed to two different providers, in the same VBP arrangement, within the reporting period submitted as a fixed-width TXT file.
Member Data, attributed to Provider 1 from 1/1/2021 to 04/30/2021
Member Data, attributed to Provider 2 from 5/1/2021 to 12/31/2021
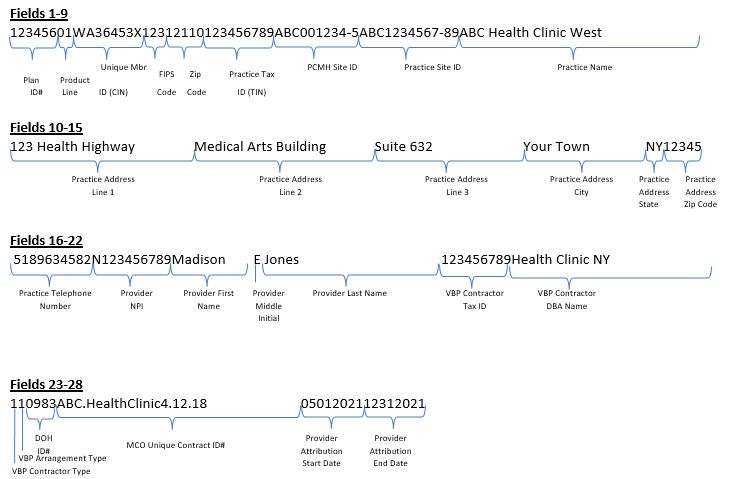
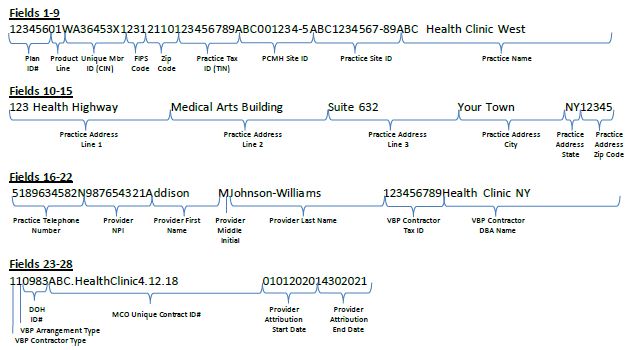
Fields 1-9:
The example below illustrates one member's data submitted as a CSV file.
| Plan ID# | Product Line | Member ID (CIN) | FIPS Code | Zip Code | Practice Tax ID (TIN) | PCMH Site ID | Practice Site ID | Practice Name |
|---|---|---|---|---|---|---|---|---|
| 123456 | 01 | WA12345X | 123 | 12110 | 123456789 | ABC001234-5 | ABC1234567-89 | ABC Health Clinic West |
Fields 10-16:
| Practice Address Line 1 | Practice Address Line 2 | Practice Address Line 3 | Practice Address City | Practice Address State | Practice Address Zip Code | Practice Telephone Number |
|---|---|---|---|---|---|---|
| 123 Health Highway | Medical Arts Building | Suite 632 | Your Town | NY | 12345 | 5189634582 |
Fields 17-24:
| Provider NPI | Provider First Name | Provider Middle Initial | Provider Last Name | VBP Contractor Tax ID# | VBP Contractor DBA Name | VBP Contractor Type |
|---|---|---|---|---|---|---|
| N987654321 | Addison | M | Johnson-Williams | 123456789 | Health Clinic NY | 1 |
Fields 25-28:
| VBP Arrangement Type | DOH VBP Contract ID | MCO Unique Contract ID# | Provider Attribution Start Date | Provider Attribution End Date |
|---|---|---|---|---|
| 1 | 0983 | ABC.HealthClinic4.12.18 | 01/01/2021 | 12/31/2021 |
TABLE 7: MCO ATTRIBUTION FILE - DATA QUALITY CHECKLIST
| Data Quality Check | Value | Notes |
|---|---|---|
| Value used for Plan_ID# is the Organization ID used to submit IDSSto NCQA | ☐ Yes ☐ No |
|
| Every record includes a valid Medicaid Client Identification Number (CIN) | ☐ Yes ☐ No |
The field is alpha-numeric and must be a valid CIN. Do not use internal organization member identification numbers. This field is mandatory for every record. |
| Total number of records submitted | ||
| Number of unique members included in file | ||
| Number of unique members by product line | MC (1) = SNP (2) = HARP (2)= |
|
| All records include a valid Practice_Tax_ID# | ☐ Yes ☐ No |
This field is mandatory for every record. |
| All records include a valid Practice_Name | ☐ Yes ☐ No |
This field is mandatory for every record. |
| All records include a valid VBP_Contractor_Tax_ID# (if the member is not in a VBP level 1 or higher then the value is set to '999999999') | ☐ Yes ☐ No |
This field is mandatory for every record. |
| For members in a VBP level 1 or higher arrangement, the VBP_Contractor_Tax_ID# represents the higher umbrella Tax ID # of the Contractor organization | ☐ Yes ☐ No |
|
| All records include a valid VBP_Contractor_DBA_Name (if the member is not in a VBP level 1 or higher than the value is set to '999999999') | ☐ Yes ☐ No |
This field is mandatory for every record. |
| Number of members assigned toeach VBP_Contractor_Type | Provider/Hospital (1) = IPA (2) = ACO (3) = Unknown (9)= |
|
| Number of members in each VBP_Arrangement_Type | TCGP (1) = IPC (2) = HARP (3) = HIV/AIDs (4) = Maternity (5) = Off Menu (6) = |
|
| Every record includes either a valid DOH_VBP_Contract_ID# OR a valid MCO_Unique_Contract_ID# | ☐ Yes ☐ No |
You must populate either the DOH_VBP_Contract_ID# field or the MCO_Unique_Contract_ID# field. Preferably both fields should be populated. If you need assistance obtaining your correct DOH VBP Contract Identifier, please email NYS DOH VBP mailbox at OQPSVBP@health.ny.gov |
TABLE 8: MLTC ATTRIBUTION FILE - DATA QUALITY CHECKLIST
| Data Quality Check | Value | Notes |
|---|---|---|
| Value used for MMIS_ID is the MLTC Plan's numeric eight-digit ID. | ☐ Yes ☐ No |
This field is mandatory for every record. |
| Every record includes a valid Medicaid Client Identification Number (CIN) | ☐ Yes ☐ No |
The field is alpha-numeric and must be a valid CIN. Do not use internal organization member identification numbers. This field is mandatory for every record. |
| Total number of records submitted | ||
| Number of unique members included in file | ||
| All records include a valid Prov_NPI number | ☐ Yes ☐ No |
The Prov_NPI is the unique 10-digit National Provider Identifier (NPI) for the provider the member was serviced by during the reporting period This field is mandatory for every record. |
| All records include a valid VBP_Contractor_Tax_ID# (if member is not in a VBP level 1 or higher, set the value to '999999999') | ☐ Yes ☐ No |
This field is mandatory for every record. |
| All records include a valid VBP_Contractor_DBA_Name (if member is not in a VBP level 1 or higher than the value is set to '999999999') | ☐ Yes ☐ No |
This field is mandatory for every record. |
| Number of members assigned to each VBP_Contractor_Type | CHHA, LHCSA (1) = IPA (2) = Hospital (3) = ACO (4) = Other (8) = NA (9) = |
|
| Every record includes either a valid DOH_VBP_Contract_# OR a valid MCO_Unique_Contract_ID# | ☐ Yes ☐ No |
You must populate either the DOH_VBP_Contract_ID# field or the MCO_Unique_Contract_ID# field. Preferably both fields should be populated. If you need assistance obtaining your correct DOH VBP Contract Identifier, please email NYS DOH MLTC VBP mailbox at mltcvbp@health.ny.gov |
| All members are assigned to only one Level 2 (or higher) VBP Contractor at a time | ☐ Yes ☐ No |

Follow Us